Nos publications

Certains se contentent d’un programme de 3 ou 4 ans pour apprendre quelque chose et certains n’apprennent jamais. Dans un monde idéal, nous sommes jugés par la qualité de notre travail et la déontologie de sa réalisation. Notre travail est le meilleur témoin à nos qualifications et non pas un papier A4 avec un tampon. Elon Musk a appris à construire des missiles (entre autre) en lisant des livres et échanger avec des connaisseurs.
Nous sommes idéalistes. Alors, nous continuons à apprendre constamment.
2007

Davarpanah M, Caraman M, Khoury P M, Augeraud E, Agachi A, Szmukler-Moncler S. L’apport de l’ancrage squelettique en orthodontie. Actualités Odonto-Stomatologiques 2007;237:41-58
Pour assurer au mieux les mouvements orthodontiques, l’orthodontie a besoin de s’appuyer sur un ancrage fiable, le plus fixe possible. Dans de nombreux cas, l’ancrage intra-buccal ou même extra-buccal ne peut répondre aux exigences d’ancrage du praticien orthodontiste. En assurant un ancrage fixe, l’ancrage squelettique permet la mise en œuvre de mouvements complexes tels que ingressions ou déplacements d’un groupe de dents. Cet article décrit l’ancrage squelettique, son développement historique, ses différentes applications, les paramètres à considérer, ses avantages puis ses limitations. Un cas clinique est présenté afin de montrer les différentes étapes du traitement ainsi que le résultat obtenu. Orthodontistes et impantologiste sont là une occasion de collaborer plus étroitement que par le passé. Cette interaction devrait permettre des traitements et des résultats considérés jusque-là comme impossibles à mener et à obtenir.
2008
L’ouvrage apporte sous une forme didactique et richement illustrée les données les plus récentes en termes de concepts, de protocoles et d’innovations technologiques.
Après un rappel des éléments anatomiques indispensables, le lecteur trouvera un premier groupe de chapitres apportant des informations scientifiques exhaustives sur la réponse physiologique des tissus durs et mous péri-implantaires ainsi qu’une description détaillée inédite des traitements de surfaces les plus récents actuellement en usage. Les informations plus cliniques sont alors abordées. Elles portent sur les formes diverses et variées des implants existant sur le marché, les critères de sélection des formes et des diamètres implantaires, les protocoles de mise en charge précoce et immédiate. Au coeur de l’ouvrage, les techniques chirurgicales et prothétiques sont détaillées, étape par étape. Elles incluent les situations particulières dans les zones postérieures où il est nécessaire de savoir quand et comment s’adapter à la hauteur osseuse résiduelle et quand mettre en oeuvre des techniques d’augmentation osseuse verticale. La maintenance et les complications chirurgicales et prothétiques sont pleinement exposées.
La dernière partie du manuel est consacrée aux avancées les plus récentes. Elle montre comment l’implantologie peut être mise au service de l’orthodontie, surtout par l’intermédiaire de l’ancrage squelettique de mini-vis « passe-partout ». Elle détaille le concept récemment introduit de platform-switching et ses résultats, les nouveaux états de surfaces rendues bioactives à l’aide des nanotechnologies ainsi que la piézo-chirurgie et ses applications.
2009
This clinical manual details the surgical and prosthetic protocols for clinicians who wish to utilize immediate implant loading in qualified patients. It details the fundamental principles, from patient selection to surgical procedures to the final adjustment of the definitive restoration. In addition, the chapters describe solutions to various challenges, such as when to use screw-retained or cement-retained provisional prostheses, how to prepare the prosthesis chairside, and when to have the prosthesis prepared in the laboratory. Including ample clinical photographs and decision-making flow charts, this comprehensive volume offers readers concrete guidelines for a proven technique that simplifies implant procedures and provides clear benefits to patients.
2010

On peut dire que le développement et la propagation de la radiographie scanner suivie du cone beam couplés à des logiciels informatiques 3D ont permis de reconstituer fidèlement sur des écrans d’ordinateur les structures osseuses des patients à réhabiliter, avec possibilité d’interaction.
L’usage de cette nouvelle technologie s’est déployé dans des applications de plus en plus avancées qui seront successivement considérées dans cet ouvrage. Quelques logiciels IAO existent sur le marché. Chacun possède sa logique et sa spécificité, c’est pourquoi, à l’instar de tout ce qui touche l’informatique, un certain temps d’adaptation et de familiarisation avec leurs fonctions est nécessaire, avant de bénéficier pleinement de toute leur puissance sur le plan clinique.
Exclusif! L’ouvrage permet d’accéder à une riche iconographie mise en ligne, venant utilement le compléter de façon dynamique et pratique: 17 vidéos en libre accès permettent au lecteur d’approfondir sa lecture.
2011
L’objectif de ce livre est de présenter les divers protocoles chirurgicaux de mise en place d’implants dans les secteurs postérieurs, en proximité des sinus maxillaires. Une description tridimensionnelle de l’anatomie des sinus guide le praticien. Indications, mise en œuvre, instrumentation, matériaux sont décrits afin de permettre à chaque praticien d’assurer une efficacité optimale.
2013

Protocoles de mise en charge et de temporisation immédiates.
Szmukler-Moncler S, Davarpanah M, Rajzbaum P, Khoury PM.
L’objet de ce chapitre est d’expliciter : les concepts sur lesquels reposent les protocoles de mise en charge immédiate ; les différents paramètres à connaître pour réaliser une mise en charge immédiate dans les conditions prévisibles ; la logistique spécifique de ces protocoles par rapport aux protocoles de mise en charge différée l’ensemble des indications qui peuvent être traitées à l’aide de ces protocoles.
2013
Immediate Implants Placed in Infected and Noninfected Sites after Atraumatic Tooth Extraction and Placement with Ultrasonic Bone Surgery
Cornelio Blus, Serge Szmukler-Moncler, Paul Khoury, Germano Orrù
Background
Only a few reports deal with implants placed in infected postextraction sites.
Purpose
Survival rates of a cohort of immediate implants cases placed in acute and chronically infected sites were compared with a cohort of noninfected ones while (1) tooth extraction and osteotomy sites were prepared with a piezosurgery device and (2) ultrasonication was applied to abate the bacterial charge at infected sites.
Materials and Methods
Eighty-six patients received 168 immediate implants distributed into three groups: noninfected (85), acute (36), and chronically (47) infected sites. Atraumatic extraction and implant osteotomy were performed with an ultrasonic surgery device without flap elevation. All sites received the same medication and surgical protocol; infected sites were ultrasonicated during 30 seconds at 72 W. Kaplan–Meyer survival rates were calculated at 1 year.
Results
The 1-year survival rates of the noninfected, chronically, and acute infected groups were 98.8, 100, and 94.4%, respectively. The differences were not statistically significant.No implant was lost after loading.All teeth and roots could be extracted in one piece. Drilling at extraction sockets was uncomplicated, without skidding.
Conclusions
Implant survival rates might be similar in infected and noninfected sites when infected sites receive standard medical and surgical treatment and are ultrasonicated. Atraumatic tooth/root extraction and implant placement can be reliably performed with piezoelectric surgery.
2014

Paradigm Shift in the Management of the Atrophic Posterior Maxilla
Rabah Nedir, Nathalie Nurdin, Paul Khoury, Marc El Hage, Semaan Abi Najm, and Mark Bischof
When the posteriormaxilla is atrophic, the reference standard of care would be to performsinus augmentation with an autologous bone graft through the lateral approach and delayed implant placement. However, placement of short implants with the osteotome sinus floor elevation technique andwithout graft can be proposed for an efficient treatment of clinical caseswith a maxillary residual bone height of 4 to 8 mm. The use of grafting material is recommended only when the residual bone height is ≤4 mm. Indications of the lateral sinus floor elevation are limited to cases with a residual bone height ≤ 2mm and fused corticals, uncompleted healing of the edentulous site, and absence of flat cortical bone crest or when the patient wishes to wear a removable prosthesis during the healing period. The presented case report illustrates osteotome sinus floor elevation with and without grafting and simultaneous implant placement in extreme conditions: atrophic maxilla, short implant placement, reduced healing time, and single crown rehabilitation. After 6 years, all placed implants were functional with an endosinus bone gain.
2015

Short Implants Placed with or without Grafting in Atrophic Sinuses: The 3-Year Results of a Prospective Randomized Controlled Study
Rabah Nedir, Nathalie Nurdin, Paul Khoury, Mark Bischof
Background
The question whether a minimal maxillary residual bone height (RBH) allows the predictable use of osteotome sinus floor elevation (OSFE) remains unresolved.
Purpose
To evaluate the efficacy of short implants placed with OSFE in an RBH of ≤4 mm and to compare bone levels around implants placed with (control) or without (test) grafting after 3 years.
Materials and Methods
Eight-millimeter implants were placed by OSFE in sinuses randomized to receive anorganic bovine bone or no grafting material. Healing time before prosthetic rehabilitation was 10 weeks. Peri-implant bone levels were measured on standardized periapical radiographs.
Results
Thirty-seven implants (17 test, 20 control) were placed at a mean RBH of 2.4 ± 0.9 mm. Three implants failed during the 3-year follow-up. After 3 years, all implants had gained endosinus bone (test: 4.1 ± 1.0 mm; control: 5.1 ± 1.2 mm; p = .001). Mean bone gain was stable between 1 and 3 years in both groups.
Conclusions
Grafting is unnecessary to achieve bone augmentation of 4.1 mm; however, more bone is gained with grafting. Bone gained over 1 year was retained. Atrophic posterior maxillae can be predictably rehabilitated using OSFE and simultaneous placement of 8-mm implants.
2015
ConsEuro 2015 – Shortlisted E-poster
Hosted by King’s College London Dental Institute.
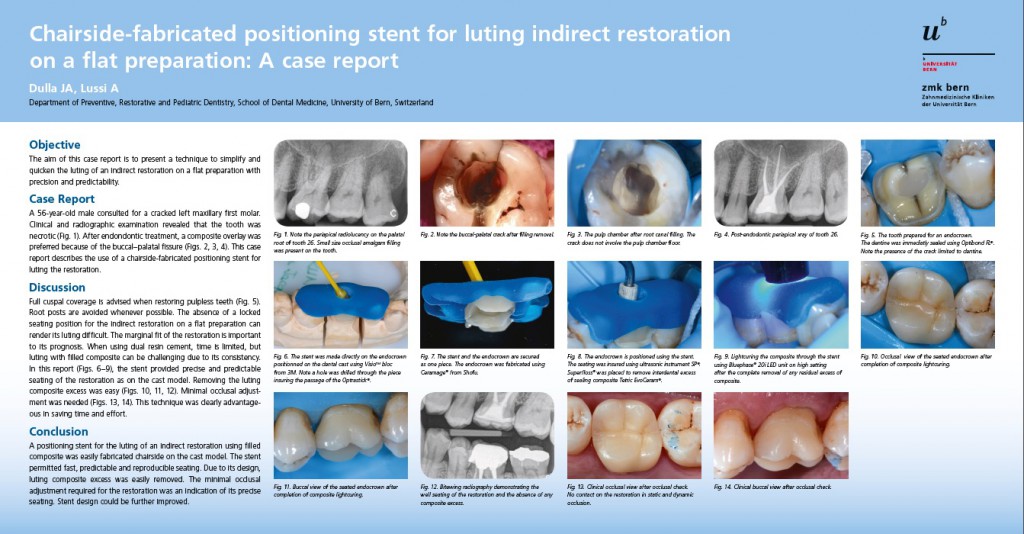
CC11 Chairside-fabricated positioning stent for luting indirect restoration on a flat preparation: A case report
Joëlle Dulla, Adrian Lussi University of Bern, Bern, Switzerland
Objective: The aim of this case report is to present a technique to simplify and quicken the luting of an indirect restoration on a flat preparation with precision and predictability.
Case Report: A 56-year-old male consulted for a cracked left maxillary first molar. Clinical and radiographic examination revealed that the tooth was necrotic. After endondontic treatment, a composite overlay was preferred because of the buccal-palatal fissure. This case report describes the use of a chairside-fabricated positioning stent for luting the restoration.
Discussion: Full cuspal coverage is advised when restoring pulpless teeth. Root posts are avoided whenever possible. The absence of a locked seating position for the indirect restoration on a flat preparation can render its luting difficult. The marginal fit of the restoration is important to its prognosis. When using dual resin cement, time is limited, but luting with filled composite can be challenging due to its consistency. In this report, the stent provided precise and predictable seating of the restoration as on the cast model. Removing the luting composite excess was easy. Minimal occlusal adjustment was needed. This technique was clearly advantageous in saving time and effort.
Conclusion: A positioning stent for the luting of an indirect restoration using filled composite was easily fabricated chairside on the cast model. The stent permitted fast, predictable and reproducible seating. Due to its design, luting composite excess was easily removed. The minimal occlusal adjustment required for the restoration was an indication of its precise seating. Stent design could be further improved.
2015

Trends of periodontal conditions in two different randomly selected Swiss (Bernese) cohorts 25 years apart
Schürch E Jr, Dulla JA, Bürgin W, Lussi A, Lang NP.
Aim
To assess the periodontal conditions of two randomly selected swiss cohorts 25 years apart.
Material and methods
Standardized examinations were performed to assess the periodontal conditions of two randomly selected populations of the canton of bern; oral cleanliness was evaluated using the plaque index (pli) and the retention index (ri). Gingival health was scored according to the gingival index (gi). Periodontal conditions were evaluated by pocket probing depth (ppd) and loss of attachment (la).
Results
At the first examination in 1985, 206 out of 350 subjects were evaluated, while in the second examination in 2010, 134 out of 490 subjects attended the examinations. In 1985, subjects showed a mean pli of 1.16, and 0.77 in 2010. Ri was 0.81 and 0.36 in 1985 and 2010 respectively. Mean gi was 1.34 and 0.6. The mean proportion of ppd ≤3 mm was 72% in 1985 and 97.3% in 2010. Ppd ≥ 6 mm affected 2.0% in 1985 and 0.3% in 2010. In 1985, subjects had an average of 20.7 teeth, while in 2010, the average was 24.6. In 1985, 7.3% of the subjects were edentulous, while in 2010, 4.5% had no teeth.
Conclusions
Trends to improvements resulting in more teeth in function and better periodontal conditions were recognized.
2018
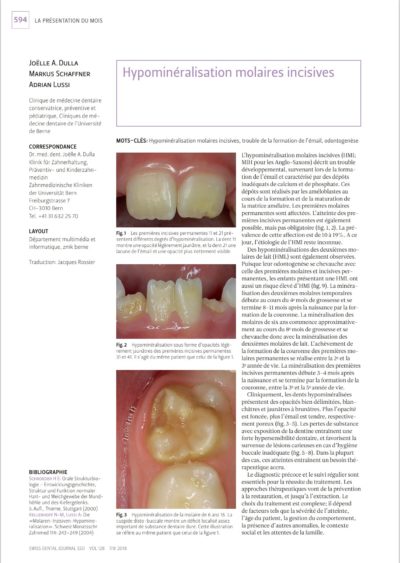
Hypominéralisation molaires incisives
Joëlle A.Dulla, Markus Schaffner, Adrian Lussi
L’hypominéralisation molaires incisives (HMI; MIH pour les Anglo-Saxons) décrit un trouble développemental, survenant lors de la forma-tion de l’émail et caractérisé par des dépôts inadéquats de calcium et de phosphate. Ces dépôts sont réalisés par les améloblastes au cours de la formation et de la maturation de la matrice amélaire. Les premières molaires permanentes sont affectées. L’atteinte des pre-mières incisives permanentes est également possible, mais pas obligatoire (fig.1,2). La pré-valence de cette affection est de 10 à19%. Ace jour, l’étiologie de l’HMI reste inconnue.
2021

Dulla JA, Meyer-Lueckel H. Molar-incisor hypomineralisation: narrative review on etiology, epidemiology, diagnostics and treatment decision. Swiss Dent J. 2021 Mar 25;131(11). Epub ahead of print. PMID: 33764036.
Molar-incisor hypomineralisation (MIH) is clinically defined as demarcated structural enamel defects affecting at least one first permanent molar with or without the involvement of incisors. It is foremost a qualitative developmental defect of systemic origin. The prevalence for MIH is estimated at 12.9% with significant differences between countries. Its etiology and pathogenesis are still not completely understood. Several environmental and medical causes have been suggested to alter enamel maturation. The hypomineralised enamel may collapse shortly after eruption and as a consequence caries lesions seem more likely to develop. Besides cavitation, hypersensitivity and/or pain are the hallmarks of clinical symptoms. Both are associated with increased dental anxiety and fear of children suffering from MIH. Consequently, patients’ care and management are challenging and necessitates a large range of non-, micro- and invasive strategies. MIH might be mixed up with three different other types of developmental defects in the enamel: fluorosis, enamel hypoplasia, and amelogenesis imperfecta. Careful diagnostic differentiation should be made before starting any dental treatment. A recent published classification system links the severity of the lesion to a treatment need index. This index is based on four values regarding two key symptoms: hypersensitivity and post-eruptiv enamel breakdown (PEB). Without PEB sealing is strongly recommended in order to prevent caries. For hypersensitive teeth as well as those with PEB use of glass ionomer cement as an intermediate cover, but mainly composite resins are materials of choice. For improvement of aesthetically compromised MIH-incisors, the resin infiltration technique has been proposed.
2021
Summary
Objectives: The purpose of this thesis is to review, analyze and summarize the published data on the skeletal, dental and soft tissue effects of Twin Block appliance in treating class II malocclusion. Its main purpose is to determine the effectiveness of the Twin Block appliance in treating Class II malocclusion, skeletally and dentally and to compare the results from prospective controlled studies and retrospective studies.
Material & methods: A thorough unrestricted electronic search of three databases (Pubmed, Google Scholar, Scopus) was performed using the designated keywords. Retrospective and prospective studies were included in this review. All papers were filed and classified in a reference management software (Papers from ReadCube). Changes (∆) to the following initial (i) measures for skeletal and dental effects were identified: ANB, SNB, SNPog; OvJ.
Results: Thirty-seven prospective and eighteen retrospective studies were included. In total, 1049 and 760 subjects were included with a mean age of 11.64 and 11.27 years in the prospective and retrospective studies respectively. The mean difference for: iANB was 6.72°, 6.29°, iSNB was 74.65° and 75.26°, and iOvJ was 9.06 mm and 8.23 mm, for the prospective and retrospective studies respectively. The mean difference for: ∆ANB was -2.33° and -2.08°, ∆SNB was +2.02° and +1.73°, and ∆OvJ was -6.07 mm and -5.23 mm for the prospective and retrospective studies respectively.
Conclusion: Both studies showed that TWB is efficient in reducing ANB and OvJ considerably, surpassing on average 2° and 6 mm respectively regardless of the average age. No statistical comparison could be made between PS and RS because of absence of control groups. Nevertheless, considering the very small difference between pooled averages, it might (or not) be statistically significant, but it is doubtful that this difference would be of any clinical significance. Overall, there was a lack of a common view of what was being measured, how and when.
2022

Conseils pour le traitement de l’hypominéralisation molaire-incisive en pratique privée
SWISS DENTAL JOURNAL SSO VOL 132 1 P 2022
Le traitement de l’hypominéralisation molaire-incisive marquée (HMI ; MIH pour les Anglo-Saxons) représente souvent un défi pour lepatient et le praticien. Des facteurs tels que l’hypersensibilité, la pulpite, les molaires HMI partiellement éruptées et les valeurs réduites des forces d’adhésion compliquent le travail médico-dentaire et en réduisent le succès à long terme. Un aspect important pour la pratique quotidienne est le fait de disposer d’un large spectre d’options thérapeutiques temporaires, également pour les dents difficiles à restaurer. Le présent travail porte sur les recommandations pratiques relatives au traitement de l’HMI. Les recommandations thérapeutiques de l’Académie européenne de médecine dentaire pédiatrique (European Academy of Paediatric Dentistry, EAPD) et des « concepts HMI de Würzburg » sont prises en compte. En complément, les méthodes thérapeutiques établies des Universités de Berne et de Zurich sont discutées